Counterfeit Pain Meds Found in Prince’s Home
/By Pat Anson, Editor
Counterfeit pain medication laced with fentanyl was found in the home of the late pop star Prince, a source with knowledge of the investigation into the his death has told the Minneapolis Star Tribune.
Prince was found dead in his Paisley Park home on April 21 and speculation immediately focused on a possible opioid overdose. A medical examiner later reported that Prince died from an accidental overdose of fentanyl, but did not say where the drug came from.
Prince did not have a prescription for fentanyl, which is used in skin patches and lozenges to treat chronic pain. He died less than a week after his private plane made an emergency landing in Moline, Illinois, where paramedics reportedly treated him for an opioid overdose.
Recently, the Drug Enforcement Administration reported the U.S. was being “inundated” with hundreds of thousands of fake pills made with illicit fentanyl, a synthetic opioid that is 50 to 100 times more potent than morphine. Dozens of deaths have been blamed on the fake pills.
The Star Tribune’s source said Prince weighed only 112 pounds at the time of his death and had so much fentanyl in his system that it would have killed anyone.
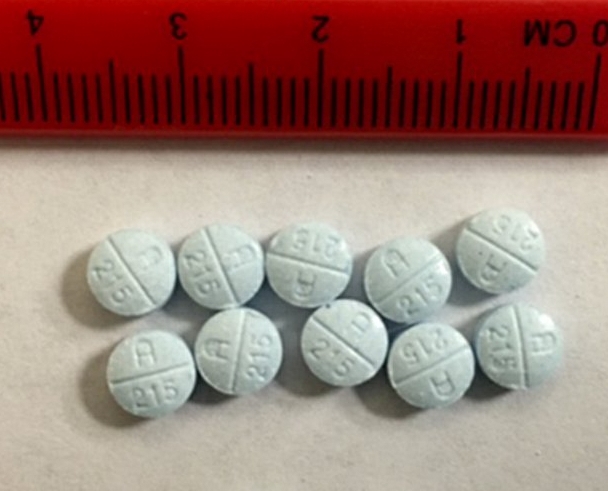
Despite the finding, investigators still aren’t sure how the 57-year-old musician ingested the fentanyl. However, they are leaning toward the theory that he took fake pills disguised as hydrocodone, not knowing they contained fentanyl, according to the Star Tribune.
If so, that would make Prince the most high-profile victim of the fast growing fentanyl crisis. Several states in the Northeast and Midwest have recently reported that most of their fatal overdoses are now caused by illicit fentanyl, not opioid pain medication.
A source told the Associated Press that several pills found in Prince’s home were labeled as “Watson 385” – a stamp used to identify generic pills containing hydrocodone and acetaminophen sold under the brand name Lortab. When one of those pills was tested, it was found to contain fentanyl and lidocaine.

The Star Tribune reported that Prince was found in his home wearing a black shirt and pants — both were on backward — and his socks were inside-out. Prince appeared to have been dead for several hours before his body was found in an elevator.
In addition to fentanyl, sources told the newspaper that lidocaine, Percocet and alprazolam were found in Prince’s system. Alprazolam is the generic name for Xanax, an anti-anxiety medication. Counterfeit versions of Xanax made with fentanyl have also been blamed on several deaths.
“The counterfeit pills often closely resemble the authentic medications they were designed to mimic, and the presence of fentanyls is only detected upon laboratory analysis,” the DEA warned in an unclassified report last month.
“Fentanyls will continue to appear in counterfeit opioid medications and will likely appear in a variety of non-opiate drugs as traffickers seek to expand the market in search of higher profits. Overdoses and deaths from counterfeit drugs containing fentanyls will increase as users continue to inaccurately dose themselves with imitation medications.”
Two public health researchers recently speculated that a “malicious actor” may be intentionally poisoning people with counterfeit medication made with fentanyl. However, a DEA spokesman said that was unlikely.
“If you’re a drug trafficker, you don’t want to poison people. You want a regular customer base,” Rusty Payne said.