Rite Aid Settles Opioid Dispensing Case
/By Pat Anson
Embattled pharmacy chain Rite Aid has agreed to a settlement with the federal government over the illegal dispensing of opioid pain medication, removing one of the last legal hurdles in the company’s bankruptcy case. Details of the settlement, which includes an explicit offer to cooperate with DEA investigations, were made public this week.
Rite Aid agreed last month to a bankruptcy restructuring plan that eliminates $2 billion in debt, while giving the company access to another $2.5 billion in loans to finance a turnaround plan. The pharmacy chain has already closed over 520 stores, about a quarter of the 2,100 pharmacies it operated prior to filing for Chapter 11 bankruptcy.
Rite Aid allegedly violated the Controlled Substances and False Claims Acts by dispensing hundreds of thousands of prescriptions for opioids and other controlled substances that lacked a “legitimate medical purpose.” The government said the prescriptions were filled by Rite Aid pharmacists from 2014 to 2019, despite “red flags” that they were suspicious or illegal.
“Pharmacies and pharmacists have an affirmative legal duty to ensure that the prescriptions they fill are legitimate,” Rebecca Lutzko, U.S. Attorney for the Northern District of Ohio, said in a statement. “When they disregard this responsibility and instead ignore red flags indicating that prescriptions for addictive painkillers are invalid, they violate the public’s trust and harm the community they are supposed to serve — all to make a buck.”
The Justice Department may have squeezed all it can get out of Rite Aid. Under the settlement, the company agreed to pay the government $7.5 million, along with an “allowed, unsubordinated, general unsecured claim” of nearly $402 million in the bankruptcy case.
An unsecured claim means the government is not entitled to any liens on liquidated Rite Aid property and has to stand in line behind other secured creditors. The $7.5 million payment may be the only one the government receives.
Rite Aid and other pharmacy chains have faced “extreme pressure” from regulators and law enforcement to rein in their opioid prescribing. According to congressional investigators, Rite Aid, CVS and Kroger allow their pharmacy staff to routinely hand over prescription records to law enforcement without a warrant. In most cases, patients are never informed that their medical records were provided to law enforcement or why they were being sought.
That cooperative relationship with law enforcement is being codified under Rite Aid’s settlement with the government. The company and the DEA have signed a memorandum of agreement “to increase communication between the company, its retailers and DEA.” The agreement requires Rite Aid to keep records relevant to DEA investigations for a minimum of five years and to give employees additional training to help them identify suspicious prescriptions.
Law enforcement agencies are not covered by the Health Insurance Portability and Accountability Act (HIPAA), which protects patient privacy.
Rite Aid also agreed to a corporate integrity agreement, which requires the company to submit data on prescriptions for controlled substances to an Independent Review Organization to determine whether the drugs are properly prescribed, dispensed and billed.
‘They Give Me the Runaround’
It’s already quite common for a pharmacist to refuse to fill an opioid prescription, regardless of a patient’s condition or need.
In 2019, a California woman with late-stage breast cancer posted a tearful video online, after a Rite Aid pharmacist said he would not refill her prescription for Norco, an opioid medication she took for cancer pain. Doyle said the pharmacist told her he was worried about being fined or losing his job if he filled her prescription, even though cancer pain is exempt from opioid prescribing guidelines.
“I have to take 20 pills a day just to stay alive,” Doyle said. “Every time I take my pain pill prescription there, they give me the runaround.”
Rite Aid eventually apologized to Doyle and offered to fill her prescriptions, but she refused to go back to the Rite Aid pharmacy where she shopped for 20 years. She died of cancer in 2020, leaving behind a 9-year-old son.
April Doyle’s case is not unique. A recent PNN survey of nearly 3,000 pain patients found that over 90% with an opioid prescription experienced delays or problems getting their medication. Nearly 20% couldn’t to get their prescription filled, in part because opioids such as hydrocodone and oxycodone are in short supply.
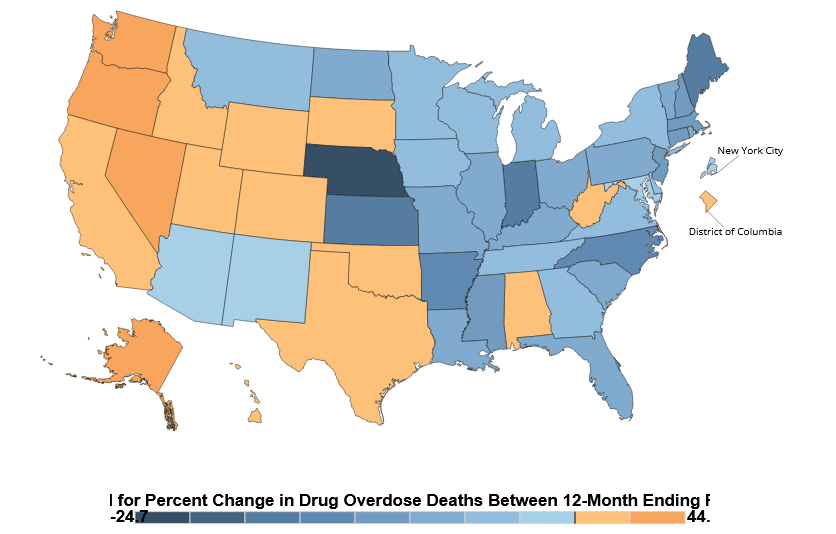
Although most U.S. drug overdoses involve illicit fentanyl and other street drugs, federal prosecutors and law enforcement continue to blame doctors, pharmacies, drug wholesalers and opioid manufacturers for the nation’s overdose crisis.
“America continues to live through the worst opioid epidemic we have ever seen. Rite Aid contributed to this crisis by ignoring obvious red flags and dispensing hundreds of thousands of unnecessary opioids,” said DEA Administrator Anne Milgram. “DEA will continue to do everything in our power to protect the health and safety of Americans and to end the opioid epidemic.”